

Background:
Lenalidomide is an immune modulator, approved for use since 2005 for the treatment of multiple myeloma (MM) patients. Its use is associated with an increased risk of infections. Combination of lenalidomide with other drugs, monoclonal antibodies, proteasome inhibitors, dexamethasone, and alkylators, can enhance the risk of serious infections. We conducted a network meta-analysis to compare the incidence of ≥Grade 3 infections among lenalidomide based regimens used in MM that can help clinicians to monitor patients for the risk of infections.
Methods:
A search was performed on PubMed, Cochrane, Embase, and Web of Science. We used the following keywords, "lenalidomide" AND "multiple myeloma" from the inception of literature till 06/10/2020. We screened 14,684 articles and included 23 randomized clinical trials (RCT) (N=11,174) in network meta-analysis. We extracted the data for serious (≥Grade 3) infections in lenalidomide based regimens. We excluded case reports, case series, preclinical trials, non-randomized clinical trials, observational studies, review articles, meta-analysis, and RCTs not providing any information about ≥Grade 3 infections. We used the "netmeta" package by Rucker et al. in the R programming language (version 4.0.2) to conduct frequentist network meta-analysis.
Results:
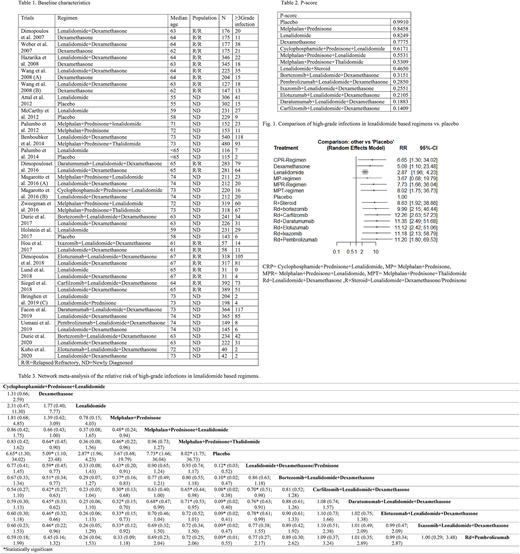
In 23 RCTs, the median age was ≥65years in 11 RCTs (N=5585) and ≤65 in 12 RCTs (5589). 9 RCTs were performed on relapsed/refractory multiple myeloma (RRMM) patients (N=4254), while 13 RCTs were performed on newly diagnosed multiple myeloma (NDMM) patients (N=6920). Lenalidomide regimen was used as maintenance therapy in 8 RCT (N=4255). Table 1 reviews the baseline characteristics. The pooled incidence of high-grade infections in trials with a median age of ≥65 and ≤65 years is 1010/5585 and 634/5589, respectively. The incidence of high-grade infections is 693/4254 in RRMM patients, 951/6920 in NDMM patients, and 466/4255 in NDMM patients with maintenance therapy.
P-score in table 2 represents the mean extent of certainty with which a regimen is better in terms of the incidence of high-grade infections, i.e., higher P-score means a lower risk of serious infections. According to P-score, lenalidomide with carfilzomib and dexamethasone is worst in terms of the incidence of infections. Indirect comparison of placebo with lenalidomide shows a risk ratio of high-grade infections of 2.87 (95% CI: 1.96; 4.23) in favor of placebo. Fig 1 outlines the indirect comparison of the incidence of high-grade infections with different lenalidomide based regimens vs. placebo.
Table 3. shows the calculated indirect comparison of high-grade infections in each lenalidomide based regimen. Heterogeneity was not statistically significant. For serious infections, lenalidomide dexamethasone showed a risk ratio of 0.86, 0.70*, 0.76*, 0.78*, 0.77, and 0.77 in comparison with the combination of lenalidomide dexamethasone with bortezomib, carfilzomib, daratumumab, elotuzumab, ixazomib, and pembrolizumab respectively (*statistically significant).
Conclusion:
This network meta-analysis suggests an increase in the risk of high-grade infections with the addition of bortezomib, monoclonal antibodies, ixazomib, and carfilzomib to lenalidomide in multiple myeloma patients with the highest increase in risk with the addition of carfilzomib. Additional randomized clinical trials are needed on the toxicity of lenalidomide based regimens to confirm these results.
Anwer:Incyte, Seattle Genetics, Acetylon Pharmaceuticals, AbbVie Pharma, Astellas Pharma, Celegene, Millennium Pharmaceuticals.: Honoraria, Research Funding, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal